
Turtles All the Way Down, translated from an anonymous Hebrew edition by Mary Holland and Zoey O’Toole, published by Children’s Health Defense, 2022
This book was written and published in Israel before the COVID pandemic. It points to the formerly dismal state of vaccine “science”, which has taken a further quantum leap into deception and censorship since 2020.
Shakespeare wrote a play called Much Ado About Nothing. There are several physics books written about The Vacuum, and there is a meditation book about Emptiness. But perhaps the most relevant analogy is the Sherlock classic about the Dog who Didn’t Bark from Arthur Conan Doyle.
It is natural to come to this book looking for scientific findings that we might weigh and evaluate and balance. But there are no such findings.
There are no competent and unbiased studies on vaccine safety, not for any vaccine. We could content ourselves with saying “we have no idea how safe these vaccines are”; or we could join Sherlock Holmes and ask, “why not?”
The situation for vaccine effectiveness is not much better. The literature is completely dominated by industry-funded “science” that is designed not to discover the truth but to sell vaccines.
This book is as frustrating as it is important.
Chapter 2
Chapter 2 is the core of the book. It carries the convincing message that “studies” of vaccine safety are propaganda, not science.
Maybe this book could be a lot shorter. Vaccine safety is not studied. Instead, deceptive study designs and reporting of the wrong statistics create an illusion that there is science behind the vaccines.
The logical conclusion is that companies that profit from vaccines have a lot to hide, but we really have no idea. The appropriate studies are not being done. The “studies” we do have are all funded directly or indirectly by the companies that produce the vaccines, and they compare side effect profiles of one vaccine to another vaccine, but they never compare side effects from vaccination to no vaccination, or even to a true placebo injection with something truly known to be harmless, like salt water.
I would go further than the authors of this book (who have remained anonymous, probably for good reason), and make two additional points about vaccine safety testing.
First, there is no justification for using any placebo in a safety study. Placebo control is used to correct for the fact that many people derive psychological benefit just from the attention and the reassurance of being treated. When studying drug efficacy, placebo controls are important. But in studying detrimental side-effects there is no excuse for using placebos. Adverse events from every drug should be evaluated in comparison to what the patient would experience if he did not receive any treatment. Placebos are unnecessary, and use of toxic placebos is clearly a sham, a ruse to hide adverse events.
The Placebo Effect
The only legitimate argument for using placebos in vaccine safety studies is that the physician caring for the patient should be blind to whether his patient is in the test arm or control arm of the study. In my opinion, this advantage is overridden by the potential for corruption. In real life, blinding of the doctors is not generally effective, and in the 2020 Pfizer vaccine trials, there was a major unblinding scandal.
Why do we trial drugs against placebos as a comparison? Because most patients get better on their own, and the fact that there is a professional treating them and concerned about their health makes it even more likely they will get better on their own. Dr Ted Kaptchuk of Harvard Medical School has made a career out of the placebo effect. Most drugs that are found to be effective and approved by FDA are actually less effective than the placebo effect, meaning that the number of people who improve with placebo alone is more than half of the number who improve from the drug. More than half of the benefit of most commercial drug treatments derives from the placebo effect. Remarkably, patients still benefit from the placebo effect even if they are told they are getting a placebo with no pharmacological activity.
Drug manufacturers regard the placebo effect as an obstacle to approval. They are looking for ways to minimize it. But from a public health perspective, “placebo effect” represents an enormous understudied resource, which may hold potential for enhanced healing if we knew how to optimize it. In other words, the mind has a substantial effect on the body, and the placebo effect is just one small window into this effect. If we could optimize the benefit of mind/body healing, we would increase the (already substantial) benefit we see in the placebo effect.
My point is that these considerations apply to efficacy, and not safety. There is no justification for using placebos in safety trials.
Proof of safety
Second, the burden of proof has been reversed in these safety trials. The proper use of the 95% confidence test would be to demand 95% confidence that the drug being tested is not causing harm. But in practice, the convention is to invert the burden of proof. In tests of drug safety, the drug is reported to be “safe” if there are “not significantly more” side effects from the test drug than the placebo. In other words, the test drug is innocent until proven guilty beyond a reasonable doubt. The new drug may have a lot more reported side effects than the control drug masquerading as a “placebo”, and statistics may demonstrate with 94% certainty that the test drug is more dangerous than the control. And yet, in these circumstances, the conclusion of the study will be that the drug is “not significantly more dangerous” than the control, simply because 94% certainty falls short of the conventional standard “p<0.05”. A technical way of saying this is that the null hypothesis is conventionally taken to be that the drug is assumed to be causing no side effects. From a public health perspective, the null hypothesis should be that the drug is dangerous until proven safe. Eπὶ δηλήσει δὲ καὶ ἀδικίῃ εἴρξειν. “First, do no harm.”
In practice, this reversal of the burden of proof has a compounding effect. Each vaccine is more dangerous than the last. Maybe the first vaccine on the schedule is pretty safe. Then it is used as a placebo in the trial of vaccine #2, and the result is that vaccine #2 is “not significantly worse”, which means it is a lot worse but statistics fall short of proving this with p<0.05. So now vaccine #2 is approved, and vaccine #3 is tested using vaccine #2 as a placebo. The result is that vaccine #3 is “not significantly worse” than vaccine #2, and so vaccine #3 is approved. This is a ratcheting down of vaccine safety standards, and it has proceeded for more than 30 years. How dangerous are the current generation of vaccines? We have no way to know.
Chapter 3
More of “we know nothing.”
The Vaccine Adverse Events Reporting System (VAERS) was launched in 1990 as a joint program of FDA and CDC. It is a voluntary system, and it takes a significant time to complete a report using clunky on-line software. Thus, busy medical professionals are incentivized not to file VAERS reports. Any medical problem that arises in the days or weeks following vaccination is invited to report to VAERS, whether or not it is proven to be caused by the vaccine. In fact, the point of VAERS is to look for statistical evidence to decide if there is a causal relationship in each particular case, for each side effect, for each vaccine.
Only a small fraction of vaccine side effects ever get reported to VAERS. This would not be so much of a problem if it were a random sample, but the underreporting rate almost certainly varies steeply with the symptom, and probably varies somewhat with the particular vaccine.
Clearly, the system is deeply flawed (by design?), but it is the system that we have, and it enables us to do at least a rough comparison of different vaccines. By this measure, the current generation of mRNA vaccines is off the charts, with about 50 times more adverse events, including hospitalizations and deaths, compared to the worst vaccines of the past.
This story emerged after the Israeli edition was published. In the book, it is reported that 20,000 to 30,000 new events are reported to VAERS each year. In contrast, there have been 1.5 million reports associated with the COVID vaccines since January, 2021, and they are overweighted in the most serious categories, including hospitalizations and deaths.
An alternative to VAERS, called VSafe, was created by CDC when the COVID vaccines were introduced, after the publication of Turtles. VSafe has different problems from VAERS, but one question that it had potential to resolve was the actual frequency of adverse events. VSafe data has been hidden from the public for nearly two years, but after a lawsuit from ICAN (Del Bigtree’s Highwire), VSafe was forced to release some data last month. As a result, we now know that 13% of vaccine recipients were sick enough to miss school or work, and 8% saw a doctor about their symptoms. This is more evidence that the COVID vaccines have been a public health disaster on a different scale from vaccines in the past.
Chapter 4
This is background material necessary to understand how the science of epidemiology works. Statistical studies over large populations are used to find evidence for a causal relationship between some behavior or intervention or condition and a disease. The chapter uses the relationship between smoking and cancer to illustrate how easy it is to game epidemiological studies to hide a relationship, even one so prominent as the fact that smoking causes lung cancer. Cigarette companies sponsored their own “studies” for decades that were designed to confuse the scientific literature. Are vaccine manufacturers doing the same thing today?
Chapter 5
How surprised should we be when the results of a scientific study turn out to support the financial interests of the company that funded the study? The problem is not that studies are biased—in fact, scientists have been looking for one result or another in their own work for as long as there have been experiments. There’s no such thing as objective science. The problem is that the the entire field of medical science has been dominated by funding sources connected to a single industry. In effect, there is no longer a forum in which competing scientists argue over their pet theories. There are only studies that support the “safe and effective” message, and no one funded or motivated to argue the opposite.
This chapter includes five case studies to illustrate ways that the scientist can put the rabbit in the hat. This was my favorite part of the book, only because I am a statistician and it constituted a master class in how to lie with statistics.
Just by the by, How to Lie with Statistics was a 1954 book by Darrell Huff which has become the all-time best selling text on basic statistical methods over the years, with more than twenty-two editions and 1.5 million copies sold of the English version alone. Rumor has it that title was spotted on the bookshelf behind Bill Gates in one of his Youtube videos.
Madsen 2002 compared the rate of autism among half a million Danish children who had received the MMR with those who did not. But instead of looking at the whole 500,000 and asking for the relative rates of autism, it looked at the small number of autistic children and asked whether they were vaccinated. This reverse logic both reduces the sensitivity of the method and makes it easy for bias to creep into the selection. There were only 53 unvaccinated children in the sample with autism. If the statistics had been done in the forward direction, this would indicate a very low background rate among the unvaccinated. But within the logic of an “association study”, there were too few children in this arm of the sample to form a statistical signal. Hence the conclusion, “This study provides strong evidence against the hypothesis that MMR vaccination causes autism.” But the vaccination status of these 53 was not confirmed, and since vaccination rates were extremely high and reporting of vaccination is lax, it is likely that some or even most of those 53 autistic children had in fact received the MMR vaccine. Even so, the unadjusted data in Madsen show a 45% greater risk of autism among the vaccinated, but after unspecified “adjustments,” the relative risk of autism was reduced below zero. This paper was highly publicized and was subsequently cited as conclusive evidence that the MMR vaccine does not cause autism.
DeStefano 2013 purported to look for a relationship between the number of vaccines that a child received and the risk of autism. But instead of actually counting the shots, they counted the “antigens”, meaning the proteins included in the vaccine that stimulate the immune system. This was a sleight-of-hand, because during the course of the study, an older tetanus vaccine was replaced with a different version. The older vaccine contained 3,000 antigens because it was based on the whole tetanus bacterium, whereas the new version injected just 6 tetanus proteins. These numbers dominated the antigen counts, so really the study ended up comparing children who got the old tetanus vaccine with children who got the newer one. The finding was that the rate of autism in children who got the new tetanus vaccine was higher than the old vaccine. But the conclusions were framed as “more vaccines lead to lower autism rate”, and that’s how the results were reported.
Grimaldi 2014 asked whether vaccination with Gardasil (HPV) vaccine contributes to autoimmunity, and like the Masden study, it worked backward from a set of children who had autoimmune symptoms, and asked how many of them had received Gardasil. In order to make a meaningful comparison, this type of study also needs a matched control group of women who did not have autoimmune symptoms. You might think the control group should have been chosen from a set of women who did not have autoimmune disease. But instead, the authors used the same database, and used as “controls” women who had a different autoimmune disease from the subjects. For example, to prove that Gardisil does not cause lupus, they chose as controls women who had Type I diabetes and asked whether more of them had received Gardisil than in the lupus group. Thus the design was blind to the possibility that Gardisil might be causing both diabetes and lupus (which, indeed, seems to be the case).
McKeever 2004 should have been the smoking gun of serious vaccine side effects for children. The raw data showed that children vaccinated with DPT (diptheria-pertussis-tetanus) were 14 times more likely to develop asthma than unvaccinated children, and those who got the MMR vaccine (measles-mumps-rubella) were 3.5 times more likely to develop asthma. But right in their opening, the authors reveal their motivation for publishing this study: “It is clearly important to gain a detailed understanding of the relationship between vaccination and allergic disease, because a perception that vaccination is harmful may have an adverse impact on the effectiveness of immunization programs.” Thus, the authors introduce the observation that unvaccinated infants see their pediatrician less often than vaccinated children. You or I might interpret this as evidence that the babies were healthier and needed less medical care. But the hypothesis of these authors was that these unvaccinated children had just as much asthma as their vaccinated peers, but it went undiagnosed because they didn’t see their doctors often enough. Conclusion: “In this observational study analyzing computerized primary care records, we found an association between MMR and DPPT vaccination and the incidence of asthma and eczema, but these associations appeared to be limited to the minority of children who rarely seek care from a GP. This limited association is more likely to be the result of bias than a biological effect.”
Fombonne 2006 “contains so many faults, it would take at least a full book chapter to detail them all,” and yet it was widely cited and the author was interviewed in multiple public appearance. The premise was that in Montreal during the years 1987-1998, MMR vaccination increased while incidence of autism decreased. But a year after publication, an independent researcher discovered that authors of the study had actually correlated autism rates in Montreal with vaccination rates in Quebec City, 150 miles away. The authors, without disclosing it, had substituted MMR vaccination rates in Quebec City for vaccination rates in Montreal.
There was no retraction. No apology. No correction from the many media outlets that had eagerly publicized the study when it was first announced.
Chapter 6
“Studies that will never be done” This chapter was an antidote to “how to lie with statistics”. It describes the straightforward ways in which the side effects from vaccines might be easily and unambiguously tested. These study designs have not been tried, or maybe the studies were done and the authors (or their employers) decided not to publish the results.
However, I know of one honest study, published after the Israeli edition of Turtles and thus not included in this chapter. Biostatistician James Lyons-Weiller worked with Portland’s pediatrician “Doctor Paul” Thomas, correlating the health of all his 3324 patients with their vaccination status. Doctor Paul is one of the few pediatricians who takes the time to explain benefits and risks of each vaccine to each parent, and lets parents consider which vaccines they want their children to receive. As a result, his practice includes a broad spectrum, from children who had the full course of recommended childhood vaccines (a small number) to children who received no vaccines at all (about ⅙). In 2020, Lyons-Weiler and Thomas published a study in which they compared health outcomes for this population of children with very different vaccination histories. For an independent variable, they chose the total number of vaccinations received by each child, and they asked whether this was correlated with the number of times the child came to the doctor with a fever or asthma or earaches or a long list of other ailments. Seventeen diseases were significantly more prevalent among the highly-vaccinated children, with high statistical confidence, most with p<0.0001. Among vaccinated children, there were more than 50 diagnosed with ADHD, but not a single unvaccinated child. The overwhelming conclusion was that “the vaccinated children appear to be significantly less healthy than the unvaccinated.”

A year after publication, the journal was pressured to retract this article, the reason given being that “Following publication, concerns were brought to the attention of the editorial office regarding the validity of the conclusions of the published research.” Can’t argue with that.
Chapter 7
The US CDC has offered a recommended schedule of childhood vaccines, and most states have taken it up. Vaccination is overwhelmingly the norm. 63% of American infants are fully compliant with the schedule. In most places, vaccination is a mandatory for public schools.
And yet, there is no research to evaluate whether there is a public health benefit or an individual benefit from full compliance compared to partial compliance compared to no vaccination at all. Most conspicuous is the absence of studies of interactions among vaccines given in the same needle, or the same day, or in close proximity. The emperor has no clothes.
Chapter 8
Part of the reason that those who profit from vaccines are able to stifle objective investigation is the widespread belief that vaccines played a decisive role in vanquishing infectious disease in the developed world over the course of the 20th Century. It is true that the burden of infectious disease was greatly diminished over this time, and it is true that vaccines played a part, especially for certain diseases, notably smallpox and diphtheria. But for the majority of diseases, the heavy lifting was done by refrigeration, better hygiene, public education, and antibiotics. This truth is attested by the fact that disease rates were already way down by mid-century when vaccination against large numbers of diseases was just starting to come into practice.
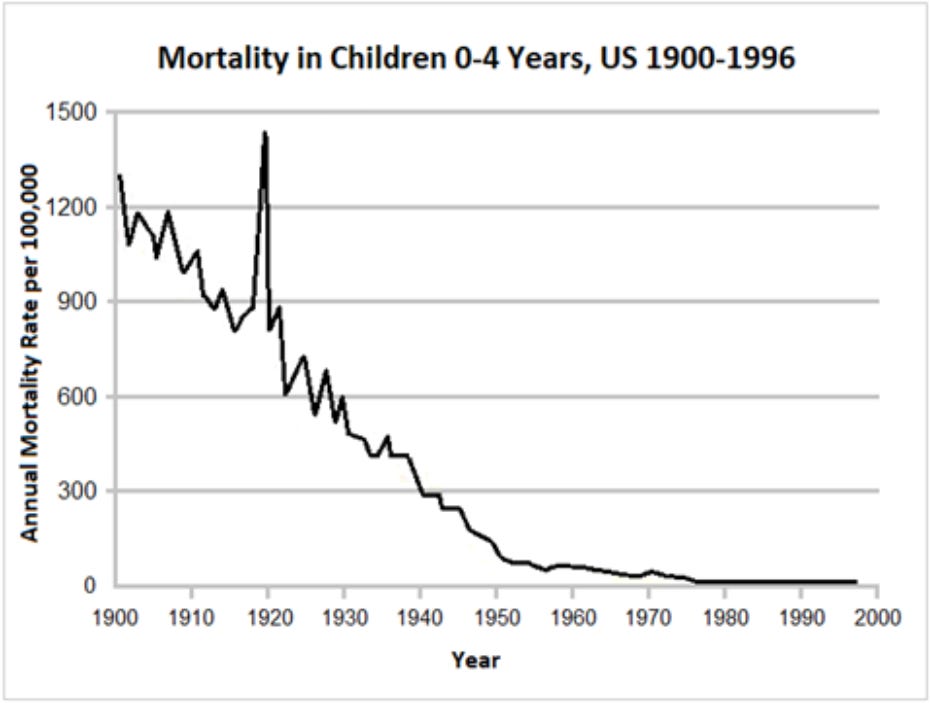
Credit: Turtles All the Way Down, p 266
Chapter 9
We might think that once the rate of spread of a disease is reduced below patient-replacement level (Ro=1), the disease is fated to disappear. And yet, despite decades of practice and high rates of vaccination, this has not happened. The reasons is that most vaccines are not “sterilizing”. That is to say, they prevent a person from having severe symptoms, and in many cases may protect against symptoms altogether. But the virus or bacteria can still replicate within the vaccinated person. He may still be a carrier, so that he can transmit to someone else a disease from which he never suffered himself.
This phenomenon is surprisingly common. The flu vaccine is a particularly egregious case, because vaccinated individuals are actually more likely than unvaccinated to transmit the disease. (This also seems to be true of the COVID vaccines.) Other vaccines that cannot prevent transmission include pertussis, diphtheria, tetanus, hepatitis, and rotavirus. Of 14 vaccines on the childhood schedule, only 5 can contribute to herd immunity. Where is the rationale for mandates?
In contrast, people who have had the disease and recovered almost always cannot serve as passive carriers in the future.
Chapter 10
Polio has a chapter to itself, because there is so much conflicting evidence and so little certainty. It appears true that both the Salk and Sabin vaccines contributed to the suppression of polio in the developed world after rates of polio had already declined significantly. And yet there is evidence that polio is not just one disease caused by one virus. Some disease that has been diagnosed as polio based on symptoms including paralysis has been caused by pesticides, and some has been spread through contaminated milk. There may be several different viruses that can cause indistinguishable disease symptoms.
This is the longest chapter in the book, devoted to a single disease, and still it reaches no conclusion.
Chapter 11
The final chapter is a summary, with conclusions, recommendations, and a call for open scientific debate. “If it weren’t for countless lives ruined…the hypocrisy displayed by vaccination’s champions would be comical.”
This is a book that should not have been necessary, if only the scientific community were doing what it is known for, and what it does best.
My thirst for scientific findings was slaked very occasionally, as the dominant message of the book was that the science is so corrupted that it is hard to know anything with confidence. We are long past attributing this to incompetence or lack of funding; the reason there is no good science of vaccine risks and benefits is that the results generated by these “studies that will never be done” would be inconvenient to some very profitable corporations (and to the government agencies that they have captured).
The book is longer than it needs to be, and you can learn what you need to know by reading the summaries that are included at the end of each chapter. But it is comprehensive, convincing, and exhaustively documented. You may get the impression from this review that the book is polemical; I’m sorry — that is my voice, and not the authors’. I think the book is quite even-handed, giving vaccines credit where credit is due.
If there is any justice in the world, this book will be a turning point in the public and scientific acceptance of universal vaccination. We urgently need an open scientific discussion over an issue so central to public health policy.
The fact that “anti-vaxxer” is a term of derision is the result of one of the most successful PR campaigns in history. We’re discouraged from asking questions or advocating unbiased clinical trials. The only acceptable position is that all vaccines are safe and effective. This is supposed to be “science”.
How did it get to be this way? An aggressive, expert, devastatingly effective campaign has been run by the same companies that brought you Vioxx and Oxycontin and Avandia. They are the biggest advertisers on TV and radio. Their financial support is crucial to the medical journals and even the medical schools. They control the narrative.
Somehow, they have convinced us that they may be completely untrustworthy when it comes to antidepressants and statins, but on the subject of vaccines, they are honest and squeaky clean.
Pfizer and Glaxo are the tobacco salesmen of the 21st Century.
A picture of BG with the statistics book :
https://media.gatesnotes.com/-/media/Images/Articles/About-Bill-Gates/Summer-Books-2015/summer-books_2015_1200px_v1.ashx