
It was January, 2020, the very beginning of COVID, when news articles began appearing that connected the genetics of the virus with gain-of-function research on bat coronaviruses at the Wuhan Institute of Virology. These speculations were put to rest by an authoritative statement in the prestigious journal Nature Medicine, echoed by a summary in Science and an unusual affidavit in the Lancet signed by an impressive list of prominent scientists. The message was dispositive: “Our analyses clearly show that SARS-CoV-2 is not a laboratory construct or a purposefully manipulated virus.” But where was the support for this confident conclusion in the article itself? The 2200 word article contained a lot of natural history and sociological speculation, but only one tepid argument against laboratory origin: that the virus’s spike protein was not a perfect fit to the human ACE-2 receptor. The authors expressed confidence that any genetic engineers would certainly have computer optimized the virus in this regard, and since the virus was not so optimized, it could not have come from a laboratory.
Of course, most readers, even most scientists, take in the executive summary and do not wade through the technical details. But for careful readers of the article, there was a stark disconnect between the Cliff Notes and the novel, between the article’s succinct conclusion and its detailed scientific content.
This was the beginning of a new practice in the write-up in medical research. Recent revelations in the Fauci/Collins emails shed light on the origins of this tactic and the motives behind it. In the past, if a company wanted, for example, to make a drug look more effective than it really was, they would choose a statistical technique that masked its down side, or they would tamper with the data.
What they would not do, in the past, was to describe the results of a statistical analysis that proves X is false, then publish it with an Abstract that claimed X is true. But this strange practice has become common in the last two years. Academic papers are being published in which the Abstract, the Discussion section and even the title flatly contradict the content within.
“Increases in COVID-19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States”
This is the title of a paper by two statisticians from Harvard School of Public Health, published on Sept 30 in the European Journal of Epidemiology. The title makes the important claim that there is no public health benefit from vaccination. COVID-19 is spreading at the same rate in different populations, unrelated to whether the population is mostly vaccinated or mostly unvaccinated. It’s a powerful counterpoint to the ubiquitous demand that more people should undergo vaccination for the sake of their community. It completely undermines the requirement of vaccination to attend meetings, concerts, theater, and other public gatherings. It says there is no legitimacy to the creeping government vaccine mandates for travel.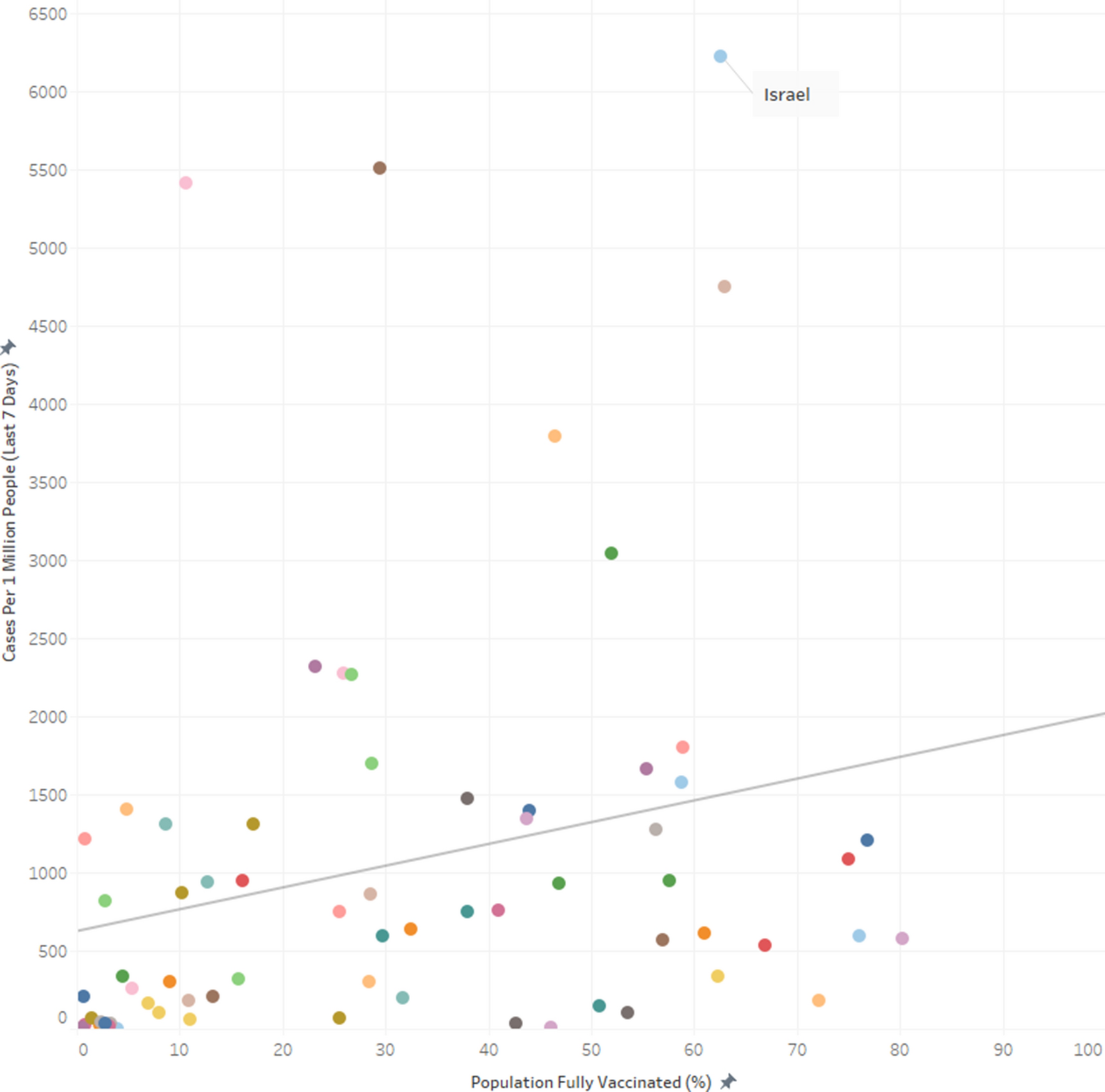
But the data in the paper don’t show that vaccination and spread of COVID-19 are “unrelated”. In fact, there is a paradoxical relationship, an insidious relationship: the more vaccinated countries had more new COVID cases (during the week when the survey was conducted). The correlation is significant (p=0.04). Still, the authors conclude by explicitly recommending propagandizing of the unvaccinated: “In summary, even as efforts should be made to encourage populations to get vaccinated it should be done so with humility and respect.”
It may sometimes be wrong to promote flawed health policy, but it’s a good thing, so long as it is done with humility and respect.
Why would these researchers take the trouble to publish data that is so damning to the vaccine narrative, and then pull punches in the title and in the conclusions? This seems to be a different case from the above, where shills for the pharmaceutical industry set out to create a deceptive narrative. I think it’s probable that in this case, soft-pedaling the implications of these glaring data may not have been the authors’ choice, but rather the journal editors’. I know from personal experience how difficult it is to get an article through peer review at most “reputable” medical journals when the results are out of sync withthe COVID narrative. It may well be that these authors fought hard to get their subversive message into print, and in order to get past peer review, they softened the language, especially, the title.
Phase I Study of High-Dose L-Methylfolate in updates Combination with Temozolomide and Bevacizumab in Recurrent IDH Wild-Type High-Grade Glioma Link
This example is unrelated to the pandemic, but it typifies a common practice in the pharma-dominated world of medical research. If a remedy is cheap and out of patent, there is no one motivated to study its efficacy. But research practice has gone well beyond neglect. In fact, they are skewing statistics to make cheap, effective treatments look ineffective if they are in competition with expensive pharma products. This is ridiculously easy to do — literally, all it requires is incompetence. Using the wrong statistical test, using a weak test when a stronger one applies, or just about any mistake in parsing the data is far more likely to make compelling data appear random than the opposite. In the case of this article, a simple B vitamin has been shown to double the life expectancy of 6 out of 14 brain cancer patients who receive it, while the other half show no benefit (and no harm).
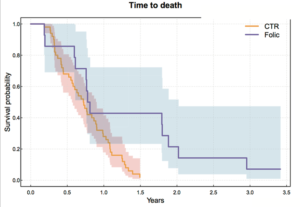
The purple jagged line extending out to the right represents 40% of patients who lived dramatically longer when treated with Methyl folate.
The abstract reports that “LMF-treated patients had median overall survival of 9.5 months [95% confidence interval (CI), 9.1–35.4] comparable with bevacizumab historical control 8.6 months (95% CI, 6.8–10.8).” The increase in median survival time is just a few months and not statistically significant. But the average survival time of the folate-treated group was more than double, and the difference was statistically significant (by my calculation, not in the article). The average is what is more commonly reported, and most readers don’t understand the difference between average and median.
The longest surviving patient on the B vitamin was still alive at the end of the study (3½ years) when every one of the patients treated only with traditional chemo was dead before 1½ years. There were three different dosages in the study, (30, 60, 90 mg) and it was not reported whether the longest-living patients were receiving the highest dosages.
This is, in fact, a hugely promising pilot study about treating a common, fatal cancer with a simple vitamin. If it were an expensive chemotherapy drug instead of a cheap vitamin, you can be sure it would have been hailed as a breakthrough. But this study will not create much excitement, and few oncologists will even know to prescribe methyl folate for their glioma patients.
Winter Statistical Report from Public Health Scotland [Link]
There is a section of this report comparing vaccinated and unvaccinated rates of disease, preceded by a warning to the reader not to take the data at face value.
“PLEASE READ BEFORE REVIEWING THE FOLLOWING TABLES AND FIGURES
There is a large risk of misinterpretation of the data presented in this section due to the complexities of vaccination data…”
The data they don’t want us to misinterpret say that people who have been vaccinated with 1 shot or 3 shots are half again as likely to contract COVID, compared to people who are unvaccinated. People who receive 2 shots are more than twice as likely to contract COVID. This is according to the authors’ own method of calculating age-standardized disease rates.

The authors emphasize that it’s not about case numbers — it’s about severe outcomes, hospitalizations and deaths.
“Evidence suggests the COVID-19 vaccines are 90% effective at preventing a severe outcome of COVID-19. COVID-19 hospitalisations and deaths are strongly driven by older age, with most deaths occurring in those over 70 years old and having multiple other illnesses. But overall, you are less likely to be hospitalised if you are vaccinated with a booster.”
What data are they talking about? Here are results from their own data table:
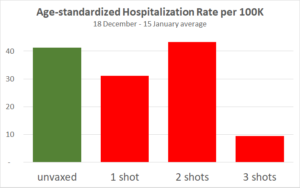
The only substantial reduction is from people who received the third shot, which has only recently been available in Scotland. For the 3-shot cohort only, vaccination effectiveness is declining over the 4 weeks. This adds to previous evidence that protection from the vaccine is short-lived, and each injection provides a shorter window of protection than the previous one. Also note that the hospitalization statistics may have been gamed.
Since the publication of this article, England but not Scotland has backed off requirements for vaccination IDs.
Clinically Suspected Myocarditis Temporally Related to COVID-19 Vaccination in Adolescents and Young Adults [link]
Myocarditis, or inflammation of the heart, is a severe and life-shortening diseases. It is virtually unknown in young people, but it is a recognized side-effect from the COVID vaccines, especially in boys and young men.
This article summarizes the experience of 139 patients who were hospitalized for myocarditis following vaccination. 19% of them were taken into Intensive Care.
“Conclusions: Most cases of suspected COVID-19 vaccine myocarditis occurring in persons <21 years have a mild clinical course with rapid resolution of symptoms.”
“Mild clinical course” — I suppose this refers to the 81% who did not go to the ICU.
“Rapid resolution of symptoms” — How would anyone know this? Myocarditis in older patients doubles the probability of death for the long term. We don’t know what it will do to young boys, because myocarditis has been unknown in this population before the mRNA vaccines. We don’t understand the mechanism by which the vaccines cause myocarditis, and we don’t know whether the mRNA permanently integrates into the human genome so that it causes ongoing production of the spike protein.
Receipt of COVID-19 Vaccine During Pregnancy
Earlier this year, MacLeod et al used data from a prominent CDC study to calculate that for women in their first trimester, the rate of miscarriage was an alarming 82%. Last week, the CDC put out a report designed to dispel our misgivings about vaccinating pregnant women. Its conclusions were unequivocal: “These data support the safety of COVID-19 vaccination during pregnancy. CDC recommends COVID-19 vaccination for women who are pregnant, recently pregnant, who are trying to become pregnant now, or who might become pregnant in the future.”
Here are three problems with the analysis of vaccine side-effects related to pregnancy.
- Concern in the past has been with the first trimester. But the report includes data only for the second and third trimesters, with less than 2% of the subjects vaccinated in their first trimester.
- Concern in the past has been with increased rate of miscarriages, but the report does not mention miscarriage, but only data about low birthweight and premature delivery.
- The last statement about what “CDC recommends” gives assurance about effects on future fertility that are not supported or even addressed by any data in the study.
|
|
population | (events per 100 live births) | Relative Risk | |
| Preterm birth | ||||
| Full population | 46,079 | 6.6 | NA | |
| No COVID-19 vaccines during pregnancy | 36,015 | 7 | Ref | |
| Any COVID-19 vaccine during pregnancy | 10,064 | 4.9 | 0.91 (0.82–1.01) | |
| mRNA vaccine, 1 dose | 1,759 | 7.7 | 0.78 (0.66–0.93) | |
| mRNA vaccine, 2 doses | 7,881 | 4.3 | 0.97 (0.86–1.10) | |
| Second trimester** | 3,668 | 6.4 | 1.05 (0.90–1.23) | |
| Third trimester** | 6,224 | 4 | 0.82 (0.72–0.94) | |
| Small-for-gestational-age at birth | ||||
| Full population | 40,627 | 8.2 | NA | |
| No COVID-19 vaccines during pregnancy | 31,699 | 8.2 | Ref | |
| Any COVID-19 vaccine during pregnancy | 8,928 | 8.2 | 0.95 (0.87–1.03) | |
| mRNA vaccine, 1 dose | 1,576 | 8.2 | 0.92 (0.80–1.07) | |
| mRNA vaccine, 2 doses | 6,982 | 8.3 | 0.98 (0.89–1.08) | |
| Second trimester** | 3,226 | 8.6 | 1.00 (0.86–1.17) | |
| Third trimester** | 5,561 | 8 | 0.93 (0.85–1.02) | |
The conclusions are expressed in terms of “relative risk”. For example, if unvaccinated mothers experience pre-term delivery 7.0% of the time, but with once-vaccinated mothers the rate is 7.7%, then the relative risk from the vaccine is 7.7% divided by 7.0%, which is RR=1.10 — a ten percent greater risk.
But that’s not the RR reported in this study. Instead they compute RR=0.78. They claim that a once-vaccinated woman is 22% LESS likely to have a problem with premature delivery. Where does this conclusion come from? No details of the methodology are provided.
However, there is a cryptic statement about a “generalized additive model for receiving 1 or 2 doses of COVID-19 vaccines.” Perhaps what they mean is that they assume for computational purposes that the risk of the first dose and the second dose are additive, so that people with two doses must be twice as likely to have a given side-effect than people who receive a single dose.
In their own data, however, people who receive one dose have higher rates of adverse outcomes in every case. If you calculate a “risk per dose”, your mathematics would force a lower risk for one dose than for two, even if reality tells you the opposite.
Why, in real life, would women who receive one dose have worse side effects? An obvious suggestion would be that the women who have adverse reactions to their first shot are likely to decline the second shot. The fact that the women chose to stop at one is telling us something that the statisticians in this study chose to leave out of their model. They probably opted out of the second shot for a reason, and that reason is likely related to their body’s sensitivity to the vaccine.
This may or may not be the correct explanation for the paradox that vaccinated women had a higher rate of complications, yet the RR is reported as if the vaccine actually lowered their risk of complications. We won’t know unless the authors choose to make their methodology public.
This report serves a purpose. People who read it superficially will find the reported results reassuring — including front-line doctors who don’t have time to evaluate the research critically. The CDC has chosen to paint over troubling safety concerns with reassuring words that are unsupported by clear science.
Conclusions
The Church was once the most trusted institution in Europe. Then the bishops started selling indulgences — a kind of get-out-of-hell-free pass for rich sinners.
Today the most trusted institution is science.
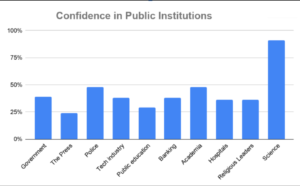
Sources: Gallup, Gallup, Gallup, Pew
This is true despite the fact that scientists are human, subject to error and to corruption. For several decades now the Church of Science has been selling indulgences. With enough money, you could buy a scientific study that says what you want it to say. Darell Huff’s book, How to Lie with Statistics was first published in 1954, and remains the all-time best-seller in its field. Recently, Gerald Posner documented the way in which the pharmaceutical industry has used their profits to affect science at every level, from medical researchers to journal editors to government regulatory agencies to the journalists who interpret science for the public.
In the age of COVID, we see two reasons that an articles conclusions might become detached from its statistical findings.
First is a shortcut by pharmaceutical companies and their shills in academia. Rigging clinical trials the old-fashioned way is expensive and time-consuming. It’s also uncertain. Sometimes the truth rears its head even if a study is designed to conceal it. Even a study that is designed to fail might succeed when the inconvenient truths are sufficiently stubborn. How much easier it is to report the results and then tack on an Abstract and a Discussion section that say what you want to say, regardless of the data tables in the body of the article!
Second is the pressure placed on independent researchers by the journal editors and peer reviewers, many of whom have ties to Big Pharma. Valid studies, honestly reported, acan be rejected for publication if they send a message that threatens corporate profits. When the researchers behind the study have some prestige and some influence, they still may find they have to soften their rhetoric in order to pass peer review.
The Nature Medicine article on the origins of the SARS-CoV-2 virus (reviewed above) seems to be an example of researcher corruption. The article in European Journal of Epidemiology, relating vaccination rates to COVID prevalence is more likely an example of corruption by journal editors and peer reviewers. For the other four articles reviewed above, I leave it to your judgment—how do you think the conclusions came to be so disconnected from the statistical findings in these same articles?
Obviously, this blatant distortion of scientific write-ups is not a long-range strategy, but the world is moving fast, and people who count on their ability to shape scientific conclusions to their financial interests will be successful for long enough to do a great deal of mischief.
What will be the damage to the credibility of Science when the dust clears?
Hi Josh,
This is Stephen Clark, senior author on the L-methylfolate paper on recurrent high-grade glioma. Thank you for your praise for this work. I too think it’s highly significant but in the process of trying to get it published the peer reviewers felt it was not significant. Regardless, I appreciate you mentioning it in your science blog.
Many thanks,
Stephen